Introduction
Skin is the human body’s largest organ, covering a surface area of about 2 sqm in an average adult. It consists of the epidermis and the dermis, deep within which are important skin appendage structures (including hair follicles, sweat glands and sebaceous glands).
Burns and their treatment have been regarded as an important medical problem since antiquity. A burn injury results from skin contact with a heat source. The factors that can cause burn injuries include high temperature, electricity, friction, radiation and chemicals . Burn injuries vary, and an increase in the body surface area affected by the burn injury affects wound morbidity and patient mortality. Other important factors directly impacting on the severity of injury include the location of the burn, temperature and time of exposure to the heat source, with a synergistic effect between them.
Burns of the hands, feet, face, eyes, ears, and perineum are always considered to be major burns.
Classification
There are 3 types of classification
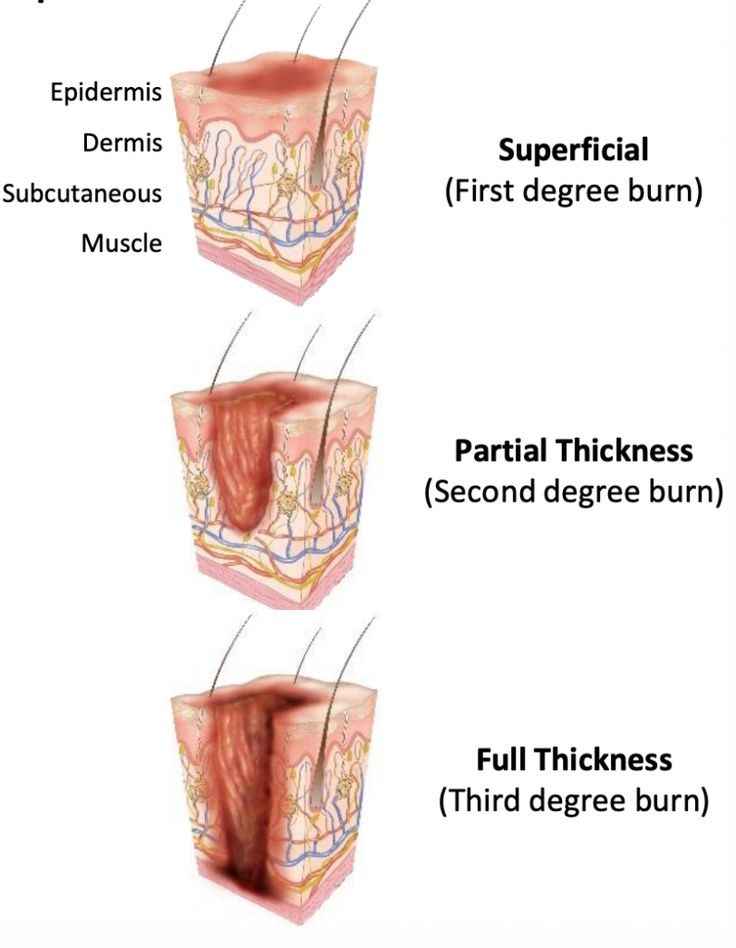
Superficial Burns
easily recognized and treated. They are painful, dry, red, and hypersensitive. Sunburn is a common example. Healing occurs with minimal damage to epidermis.
Partial Thickness Burns
are sub grouped as superficial or deep, depending on appearance and healing time. Each subgroup is treated differently.
Superficial Partial Thickness Burns
Superficial Burns are red and often blister.
Deep Partial Thickness Burns
Deep partial-thickness burns are white and dry, blanch with pressure, and the involved skin has decreased sensitivity to pain.
Full Thickness Burns
Full-thickness burns affect all epidermal and dermal elements, leaving devascularized skin. The wound is white or black, dry, depressed, leathery in appearance, and without sensation. Unless skin grafting is provided, the scar will be hard, uneven, and fibrotic. Deep full thickness, or subdermal, burns are the most severe, extending through all layers of skin as well as into the underlying fascia, muscle, and possibly bone.
Management
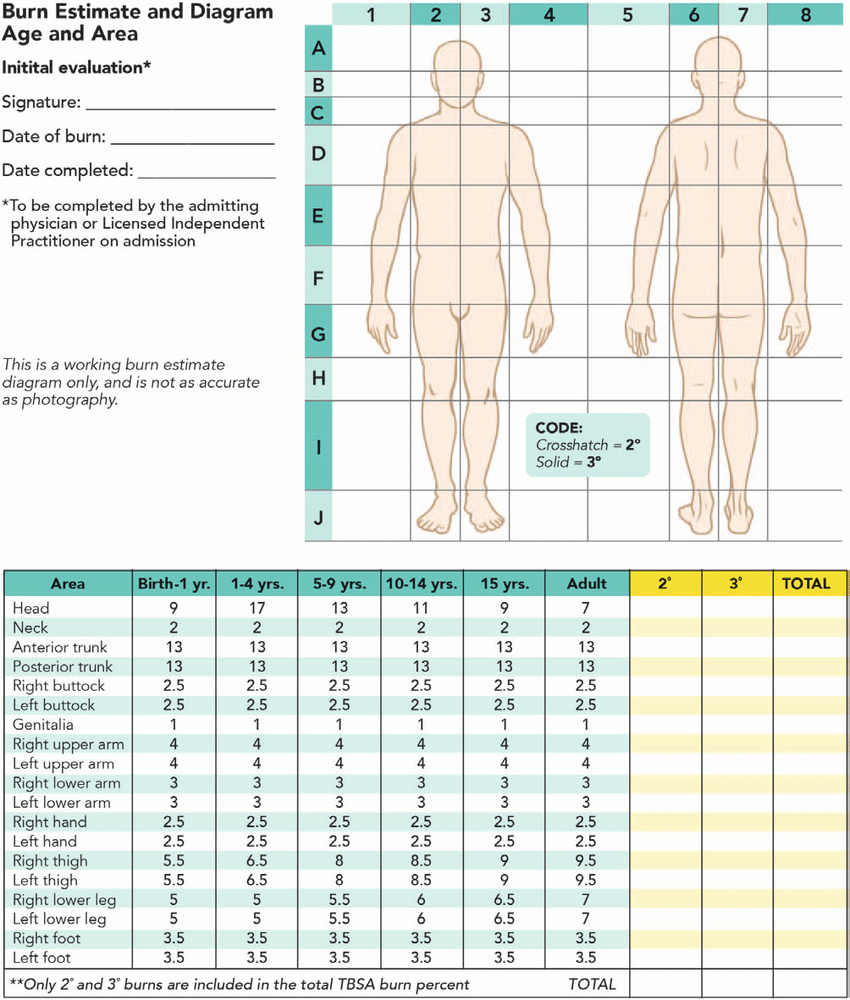
Management also depends on the depth and extent of injury. Burn extent can be classified as major or minor. Minor burns are less than 10% of the body surface area for superficial and partial-thickness burns, or less than 2% for full-thickness burns.
Steps Of Management
- ABC management
- Early establishment of an artificial airway is critical with oral or nasal burns because of their association with inhalation injuries and critical airway narrowing.
- Fluid Therapy– Parkland formula The Parkland formula for fluid therapy is 4 mL/kg/% body surface area burned for the first 24 hours, with half in the first 8 hours, in addition to maintenance rates.
- Indications for admission;
- Major burns as previously defined, uncertainty of follow-up
- Suspicion of abuse
- Presence of upper airway injury, explosion, inhalation, electrical or chemical burns, burns associated with fractures, or the need for parenteral pain control.
- Children with chronic metabolic or connective tissue diseases
- Infants deserve hospitalization
- Children with subdermal burns require immediate hospitalization at a burn center under the care of a burn specialist, fluid resuscitation
- Debridement of the wound, and placement of temporary wound coverage.